The weeks following HIV infection are a highly dynamic period, with a series of virologic and immunologic events having occurred prior to the onset of clinical manifestations of PHI and the emergence of positive findings on diagnostic tests. An exceedingly high plasma HIV viral load and rapid loss of CD4+ T cells in all tissue compartments accompany the clinical manifestations of PHI. Resolution of symptoms is associated with the development of an anti-HIV immune response and early control of viraemia1.
HIV infection occurs most commonly at the genital or anal mucosa via the dendritic cells and macrophages that populate these tissues2. The virus uses its envelope protein, gp120 to bind initially to CD4 and then subsequently to one of two co-receptors, CCR5 or CXCR4, on the cell surface of dendritic cells and macrophages. These events lead to conformational changes in the associated transmembrane protein in gp41, leading to fusion of viral and target cell membranes followed by endocytosis of the virus into the cell. Infection is typically established by virus that utilises the co-receptor CCR5 for cellular entry, which is particularly abundantly expressed by cells in the mucosal immune system. Individuals who are homozygous for a non-functional allele of CCR5, referred to as CCR5 (delta), are therefore highly resistant to infection3.
Dendritic cells may harbour the virus with or without being productively infected. Via their normal role as antigen presenting cells, these cells travel to regional lymph nodes and, through the hijacking of the normal physiological function of antigen presentation to T cells, transfer virus to multiple CD4+ T cells, rapidly amplifying the infection within lymph nodes and other secondary lymphoid structures in the mucosa, where virus is detectable within 2 days1, 4. This triggers both an antibody and T cell response with the resultant preferential infection of follicular CD4+ T cells within lymph nodes. Once virus-infected cells enter the lymphatics, there is rapid onset of viraemia, and dissemination to multiple organs, including the spleen and central nervous system5.
Cell-mediated immune responses against HIV
In contrast to the rapid depletion of CD4+ T-cells in early HIV infection, CD8+ T cells increase rapidly, up to tenfold, during this period. Cytotoxic T lymphocyte (CTL) responses of CD8+ T cells are critical in controlling viral replication in early HIV infection, through lysis of infected cells, leading to plasma viraemia being reduced to a ‘set point’ level, representing the balance between viral replication and immune control (Figure 1). This early viral set point, which occurs at 3-6 months post infection, has been shown to be highly predictive of the later course of the disease-free period until the onset of AIDS6-8. Interestingly, most of the CD8+ T cells are not specific to HIV antigens, and those that are respond to a small number of epitopes in a hierarchical immunodominance pattern. Although this response broadens over time, the CTL response later in infection seems to be less effective in controlling the disease, perhaps due to accumulation of immune escape mutations in the virus over time.
HIV selectively infects and destroys memory CD4+ T cells in early infection, with rapid depletion of these cells in the lymphoid tissues, gut and genitourinary tracts9. If not reversed early, this damage leads to distortion of the architecture within lymphoid tissues and then fibrosis, which is difficult to reverse. This results in impairment of immune responses not only to HIV, but to other antigens as well, eventually leading to the profound immunodeficiency of AIDS. Nevertheless, a robust CD4+ T cell response in PHI occurs simultaneously with, or even before, the CD8+ T cell response and is associated with maintenance of effective immunity10. The role of helper CD4+ T cells is likely performed through cytokine release, maximizing of CTL responses via interferon-gamma and interleukin-2 (IL-2) and prevention of T cell exhaustion via IL-2111, 12. The ability of CD4+ T cells to provide effector function declines as cell numbers deplete. However, in elite controllers, those rare individuals capable of persistently suppressing HIV replication in the absence of ART, the effectiveness of the CTL response is linked to preservation of the CD4+ helper T cell response10.
Some infected CD4+ T cells become resting cells before the virus causes cell death. This allows the integrated virus to become latent, establishing a viral reservoir that can be reactivated at a later time point. This reservoir is established within the earliest days of primary infection and persists for the lifetime of the patient, but can be limited in its size by early initiation of ART13.
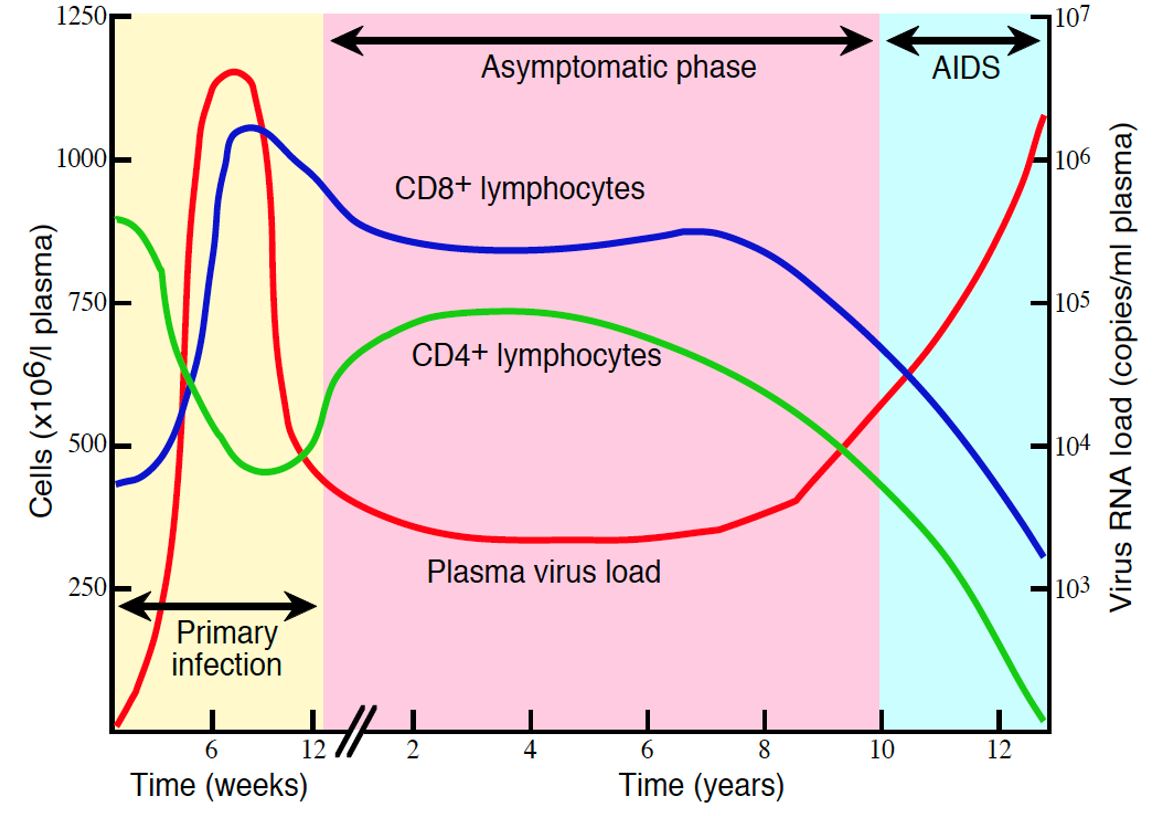
Figure 1. Time course of viral load, CD4+ and CD8+ T cell counts during HIV Infection. Adapted from “Cytotoxic T lymphocyte responses to human immunodeficiency virus: control and escape.” Sewell et al, 2000, Stem Cells, 18(4):230-44. ISSN: 10665099.