Epidemiology and Risk factors
Chronic obstructive pulmonary disease (COPD) is a slowly progressive respiratory disorder that is characterised by incompletely reversible chronic airflow obstruction(18). Smoking is the main risk factor. Other risk factors include occupational exposure to dust and chemicals, indoor air pollution or rarely genetic alpha-1- antitrypsin deficiency (19). Active smoking and frequent exacerbations due to lower respiratory tract infections contribute to progressive disease. COPD encompasses two main entities, namely 1) chronic bronchitis which refers to an obstructive ventilatory pattern that is defined by the existence of chronic bronchitis with permanent obstructed of airways (forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) ratio <70%) and 2) emphysema which is defined at the anatomical level by destruction of the walls of the alveolar sacs/ducts beyond the terminal bronchiole with an abnormal increase in size of distal airways. Both entities often occur together in patients with COPD and cause a chronic respiratory disorder(19, 20).
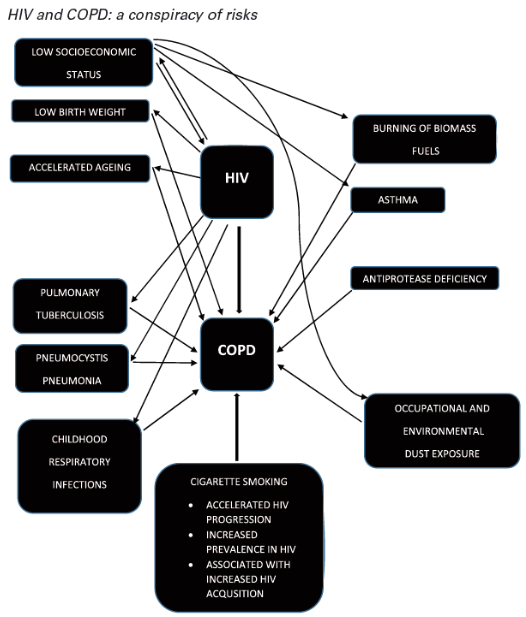
The global incidence of COPD has increased significantly in the last decade. It is now the third leading cause of death worldwide, causing 3.2 million deaths in 2019 (18). In recent years, the risk of people with HIV developing COPD has increased. Improved survival of people with HIV due to the widespread use of combined anti-retroviral therapy has meant that COPD has emerged as a disease of concern in this population (21, 22). A systematic review and meta-analysis by Bigna JJ et al on the global prevalence of COPD in HIV population demonstrated that the prevalence of COPD varied from 5.6%-10.6% depending on the diagnostic criteria used. Generally diagnostic criteria that used CT scans showed higher prevalence than those that used spirometry. There was an association between HIV infection and COPD even after adjusting for tobacco consumption status (23) . This association was postulated to be caused by a complex interplay of various mechanisms including increased susceptibility to lung infections and colonisations, inadequate inflammatory response, increased oxidative stress, accumulation of cytotoxic lymphocytes in the lung tissue and recurrent pulmonary infections, particularly tuberculosis (Fig 1) (22).
In a study by Crothers et al, 1,014 veteran affairs cohort of HIV-infected persons and 713 HIV-uninfected cohorts were followed up for their COPD diagnosis. HIV remained an independent risk factor for COPD diagnosis by ICD-9 codes (odds ratio [OR]=1.47;95% confidence interval [CI]=1.01-2.13) and self-report (OR:1.58;95%CI:1.14-2.19). Though this study did not use spirometry to confirm the diagnosis of COPD, the results of this large study validates other smaller single or multicenter studies where spirometry was measured(24). With regards to local prevalence in Australia, the Pulmonary Substudy of the Strategic Timing of AntiRetroviral Treatment (START) trial which included subjects from Australia amongst other countries in Europe and Israel reported a rate of 9.1% based on spirometry results. Cigarette smoking and age were significant risk factors for COPD in this population (25).
The association of HIV and COPD in Sub-Saharan Africa is not well understood, despite the high prevalence of HIV in the region. There is paucity of data with a few published studies suggesting a higher prevalence (26). A study from Uganda revealed a prevalence rate of COVID of 16.2% in the HIV population without significant gender difference. A large proportion of the population with COPD in this study were non-smokers. The main risk factor in this population included exposure to biomass, in poorly ventilated indoor kitchens. This also provides a plausible explanation for higher incidence rates in women and children. Biomass exposure is a known risk factor for COPD, particularly in low-income countries(27). A community-based prevalence study in South Africa (SA) confirmed a high COPD prevalence of 23.1% in adults aged >40 years. It is postulated that in addition to smoking, other airborne exposures and a history of previous tuberculosis were all risk factors (28). Additionally, in low-income countries other factors related to low socioeconomic status, eg. Pre and post-natal exposures to causative agents, nutritional deficiencies and low BMI may contribute to the development of COPD (22).
Figure 1. Complex interplay of risk factors between HIV and COPD.