The primary goal of therapy is to cure HCV, defined by achieving SVR. There are multiple clinical benefits in achieving SVR including: preventing further transmission of HCV; preventing complications of HCV-related liver disease, such as hepatic inflammation, fibrosis, cirrhosis, and HCC, and extrahepatic diseases; it reduces all-cause mortality; improves individual quality of life and removes the social barriers that the stigma of having chronic HCV can lead to. HCV cure should include a collaborative and multidisciplinary approach, consisting of therapeutic treatment and readily available access to peer support; alcohol and drug counselling; and HCV transmission education programs. Education on the importance of adherence to treatment should be emphasised and should be done for every patient prior to treatment commencement.
Cure is defined as an undetectable HCV RNA in plasma or whole blood, tested at 12 (SVR12) or 24 weeks (SVR24) post completion of treatment course. Both endpoints are considered acceptable, however, there is emerging data that has shown an undetectable HCV RNA after only 4 weeks post completion of treatment (SVR4) can strongly predict the SVR12 result, thus providing an opportunity to test at any time point after 4 weeks25,26. SVR4 testing would be ideally suited and considered adequate in population groups considered high risk of being lost to follow up, such as those incarcerated but with release imminent.
HCV treatment should be considered for all people with current HCV.
Timing of therapy
Initiation of treatment should never be delayed, especially in people with HCV infection and those who have cirrhosis. Even if the remaining staging of liver disease workup has not yet been completed, this should not delay early initiation of treatment, and the rest of the workup may be scheduled concurrently or post-treatment completion. In patients with HIV-HCV, the general recommendation is that HIV should be fully suppressed and any HIV-related opportunistic infection treated, before initiating HCV treatment with DAA therapy15.
Prior to treatment initiation, a thorough review of the patient’s medication list to identify any potential drug-drug interactions should be performed. This includes all prescribed medications, over-the-counter preparations, and recreational drugs. The possibility of drug-drug interactions should be assessed prior to treatment using the University of Liverpool’s Hepatitis Drug Interactions website (www.hep-druginteractions.org). Identified interactions require clinical evaluation and decision regarding whether certain drugs are necessary and whether they can be temporarily stopped or switched to an alternative during the treatment period15,18.
Treatment selection
The current PBS-subsidised DAA treatment available in Australia includes: sofosbuvir plus velpatasvir (NS5B nucleotide inhibitor plus NS5A inhibitor), glecaprevir plus pibrentasvir (NS3 protease inhibitor plus NS5A inhibitor), and sofosbuvir plus velpatasvir plus voxilaprevir (NS5B nucleotide inhibitor plus NS5A inhibitor plus NS3 protease inhibitor). All three DAA combination regimens are pan-genotypic.
The Australian recommendations for the management of hepatitis C virus infection: a consensus statement (2022) provides a very comprehensive review of the recommended treatment regimens to which this chapter will base its summary of recommendations from (Table 1)15. First-line combination therapy for treatment-naïve people with compensated and decompensated liver disease living with HCV are sofosbuvir plus velpatasvir or glecaprevir plus pibrentasvir. For people who are non-responders to first-line combination treatment therapy of sofosbuvir plus velpatasvir or glecaprevir plus pibrentasvir, defined by a detectable HCV RNA despite treatment completion with first-line therapy, then a triple combination regimen of sofosbuvir plus velpatasvir plus voxilaprevir should be considered.
| Treatment duration | ||||
|---|---|---|---|---|
| Regimen | HCV genotype | Pill number | No cirrhosis | Cirrhosis |
| First-line regimens for people who are treatment-naive | ||||
| Sofosbuvir 400 mg, orally, daily + Velpatasvir 100 mg, orally, daily |
1–6 | 1 pill daily | 12 weeks | 12 weeks |
| Glecaprevir 300 mg, orally, daily + Pibrentasvir 120 mg, orally, daily |
1–6 | Once daily (3 pills) | 8 weeks | 8 weeks* |
| Regimen for people who do not respond to first-line therapy due to virological failure | ||||
| Sofosbuvir 400 mg, orally, daily + Velpatasvir 100 mg, orally, daily + Voxilaprevir 100 mg, orally, daily |
1–6 | 1 pill daily | 12 weeks | 12 weeks |
| HIV = human immunodeficiency virus. * A treatment duration of 12 weeks may be considered for patients with compensated cirrhosis, at the discretion of the prescriber. |
||||
Sofosbuvir (NS5B inhibitor) / velpatasvir (NS5A inhibitor)
Sofosbuvir (400 mg) plus velpatasvir (100 mg) is a fixed-dose combination formulated into a single tablet and administered once daily. It is considered safe in patients with cirrhosis. The recommended treatment duration is 12 weeks for all patients, irrespective of whether they have cirrhosis or not. Treatment with weight-based ribavirin, in addition to sofosbuvir plus velpatasvir, is recommended in patients with decompensated liver disease as it is shown to be associated with increased rates of SVR15.
Sofosbuvir plus velpatasvir is generally well tolerated with the most frequently reported adverse events including headache, fatigue, nausea, and nasopharyngitis27. It is also considered safe to be prescribed in patients with end-stage renal disease (ESRD) without need for any dose adjustments.
Glecaprevir (NS3 protease inhibitor) / pibrentasvir (NS5A inhibitor)
Glecaprevir (300 mg) plus pibrentasvir (120 mg) is a fixed-dose combination formulated into three tablets containing 100 mg of glecaprevir and 40 mg of pibrentasvir, administered as a once daily dose with food. Benefits to glecaprevir plus pibrentasvir is that treatment duration is shorter compared to sofosbuvir plus velpatasvir, at 8 compared to 12 weeks, for both patients who are treatment-naïve with or without compensated cirrhosis. A shorter treatment course is particularly beneficial in at-risk population groups considered high risk of being lost to follow-up and who would benefit with a shorter duration of treatment.
However, the use of glecaprevir plus pibrentasvir is contraindicated and should not be prescribed in patients with decompensated cirrhosis and in patients who are compensated but have had previous episodes of decompensation. This is because protease inhibitor-containing regimens are associated with higher protease inhibitor concentration and therefore, a higher risk of hepatic toxicity18.
Glecaprevir plus pibrentasvir is otherwise well tolerated in people with compensated cirrhosis and those without, with the most frequently reported adverse events being fatigue, headache, and nausea28. Glecaprevir plus pibrentasvir is recommended first-line treatment for people with end-stage renal disease, including those on dialysis15.
Sofosbuvir (NS5B inhibitor) / velpatasvir (NS5A inhibitor) / voxilaprevir (NS3 protease inhibitor)
Sofosbuvir (400 mg) plus velpatasvir (100 mg) plus voxilaprevir (100 mg) is a fixed-dose triple-combination formulated into a single tablet and administered once daily with food. This regimen is reserved for people who fail to respond to first-line sofosbuvir plus velpatasvir or glecaprevir plus pibrentasvir as a salvage therapy and is not PBS-approved for treatment-naïve people. Recommended treatment duration is 12 weeks for all patients with or without cirrhosis.
Sofosbuvir plus velpatasvir plus voxilaprevir is also generally safe and well tolerated in people with compensated cirrhosis and in those without. The most frequently reported adverse events were headache, asthenia, nausea, fatigue, and diarrhoea. However, none of these adverse events reported frequency were >10%29.
Pregnancy and breastfeeding
There is a current paucity of published data on the safety and efficacy of HCV treatment in pregnant women and therefore treatment with DAA therapy is not recommended. All available PBS-listed DAA treatments are classed as Category B1. Ribavirin is a definite contraindication in pregnant women due to its teratogenicity risk and people on ribavirin should be counselled and put on contraceptive precautions during treatment and for 6 months post-treatment.
There is also limited published data on breastfeeding safety while on DAA treatment and is therefore also not recommended at this stage. However, there are no contraindications to breastfeeding in people with HCV with available data not showing any risk of mother-to-child transmissions30.
On-treatment monitoring
In treatment-naïve people with compensated cirrhosis or without cirrhosis on DAA therapy, extensive monitoring while on treatment is generally not required. Recommended follow-up requires a review at least 12 weeks after completion of therapy to test for SVR. However, more regular follow-up intervals can be tailored in certain populations who are considered at-risk, to optimise treatment adherence, monitor for any adverse events and potential drug-drug interactions.
In people who are also receiving ribavirin, they do require regular monitoring of haemoglobin levels. In addition, these patients will generally have hepatic decompensation and so regular follow-up and serological liver function test monitoring is recommended.
HCC surveillance with 6-monthly liver ultrasound is recommended in all patients with cirrhosis. If HCV treatment was commenced on first diagnosis of cirrhosis, then a baseline liver ultrasound should be performed.
In the event of incomplete DAA adherence, this should be documented and its management algorithm will be addressed in the following section.
Management of incomplete DAA adherence
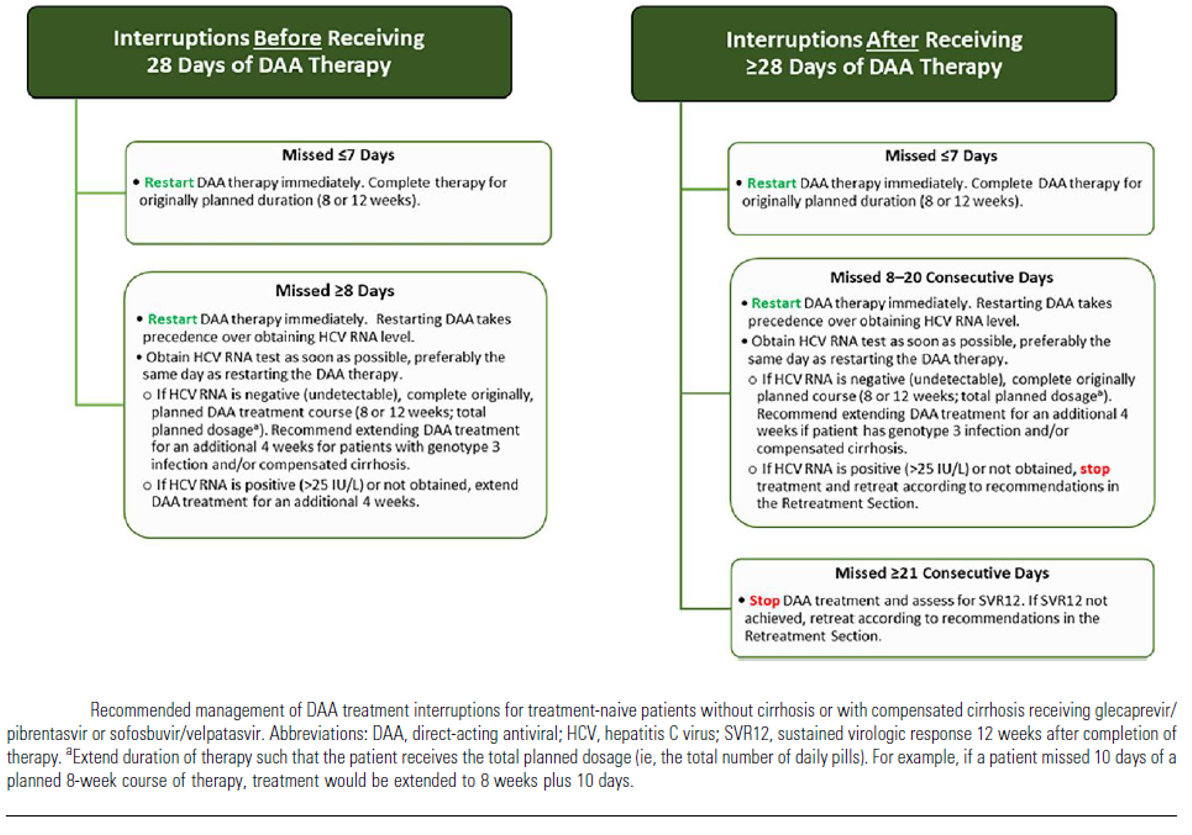
Poor adherence and an incomplete treatment course are relatively common, occurring in 11% to 40% who start treatment31-33. A risk assessment should always be an important consideration whenever someone is starting DAA therapy. In the event of treatment interruption, AASLD has developed a guidance statement on the management of DAA treatment interruptions in treatment-naïve patients, without cirrhosis or with compensated cirrhosis, receiving sofosbuvir plus velpatasvir or glecaprevir plus pibrentasvir (Figure 1)19, and the recommendations are in accordance to whether treatment interruption occurred before or after receiving 28 days of DAA treatment.
Interruptions before receiving 28 days of DAA therapy
If treatment has only been missed for ≤7 days, then treatment can be immediately restarted, and the patient should complete therapy for the originally planned duration.
If therapy is missed ≥8 days, then restart treatment immediately, but obtain an HCV RNA preferably on the same day of restarting. Restarting DAA should always take precedence over obtaining a repeat HCV RNA level. If the HCV RNA is undetectable, then the patient should complete the originally planned treatment duration. However, treatment extension for an additional 4 weeks (in addition to the originally planned duration) is recommended in patients with genotype 3 infection or compensated cirrhosis (regardless of HCV RNA status) and in all patients with a detectable HCV RNA.
Interruptions after receiving ≥28 days of DAA therapy
If treatment has only been missed for ≤7 days, then treatment can be immediately restarted, and the patient should complete therapy for the originally planned duration.
If therapy is missed between 8-20 days, then restart treatment immediately, but obtain an HCV RNA preferably on the same day of restarting. Restarting DAA should always take precedence over obtaining a repeat HCV RNA level. If the HCV RNA is undetectable, then the patient should complete the originally planned treatment duration. Treatment extension for an additional 4 weeks (in addition to the originally planned duration) is recommended in patients with genotype 3 infection or compensated cirrhosis. However, if HCV RNA is detectable >25 IU/L or not obtained, then treatment should be stopped and retreatment needs to be prescribed.
When therapy is missed for ≥21 consecutive days, then treatment must also be stopped and SVR12 tested. If SVR12 is not achieved, then retreatment needs to be prescribed.
Post-treatment follow-up in population groups who achieve SVR
Patients without cirrhosis and who achieve SVR can be considered definitively cured from HCV. However, patients with advanced fibrosis (METAVIR score F3) or cirrhosis (METAVIR score F4) and who achieve SVR are recommended to continue indefinite HCC surveillance with liver ultrasound every 6 months15,18.
In patients with pre-existing cofactors for liver disease, such as alcohol misuse disorder or metabolic risk factors for MASLD such as obesity, type 2 diabetes, hypertension, and dyslipidaemia, should be further evaluated +/- referral to a hepatology specialist.
People with a history of PWID, and recent or current PWID on opioid substitution therapy (OST), are recommended for at least annual HCV testing and also after any high-risk episode in PWIDs. The basis of this recommendation is due to the high prevalence of infection and reinfection in this population cohort.
People with HIV should have serological screening for HCV every 12 months. In people who are considered at high-risk of reacquisition of HCV, then they should have 3-6 monthly liver function test screening. A repeat HCV RNA should be performed whenever there is an unexplained transaminase level derangement.
Summary
Concurrent HCV-HIV is common and has historically contributed to the heavy burden of comorbidity and premature mortality for this population group. The currently available PBS-subsidised DAA treatment in Australia now offers a cure for the vast majority of those living with HCV, with added benefits in those also living with concurrent HIV in reducing the likelihood of liver disease progression.