Cervical cancer is the 14th most commonly diagnosed cancer among women in Australia with an age standardised incidence rate of 6.8/100,000 in 2013 (5, 6). Almost all (99.7%) cervical cancers have HPV detected in biopsy specimens (7). Cervical cancer incidence starts to rise in women in their late 20s with 30% of cases occurring in women under the age of 45 and the highest burden being in women over 45 years of age (8). There is a second peak of disease in the age group of 60-65 years.
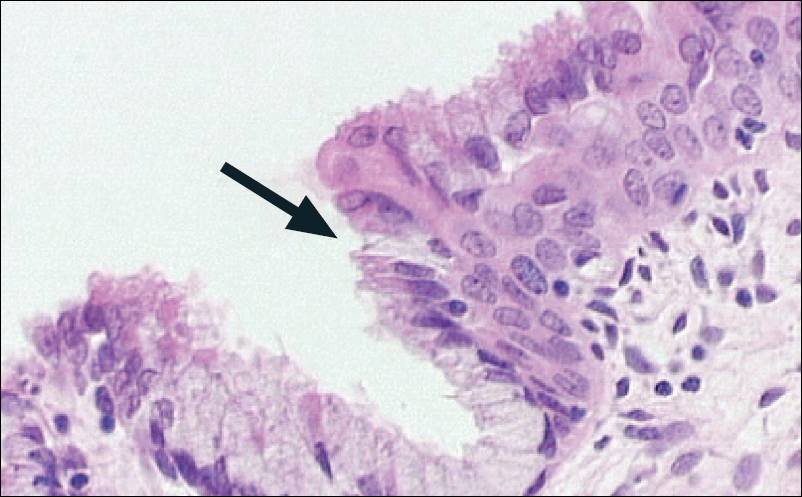
The cervix is particularly vulnerable to the effects of HPV infection at the transformation zone (Figure 1), where the stratified squamous cells of the vagina change to become the columnar cells lining the endocervix and uterus, and most HPV-associated cervical lesions occur within this area (9). Infection in the general population is extremely common with up to 60% of sexually active adults acquiring HPV infection within 36 months of commencing sexual activity and an annual incidence of 14% (10). Other studies have demonstrated a cumulative incidence of up to 60% over 5 years (11). The lifetime risk of acquiring an HPV infection is estimated to be 80% (12-15). The majority of individuals infected with HPV clear the infection within 12-24 months (16, 17). However, persistence of HPV may lead to the development of intraepithelial neoplasia (IN), which is the cancer precursor (18, 19). HPV 16 is a particularly virulent genotype (20, 21), with a lower clearance rate than other HPV types (22) and a higher likelihood of progression to precancerous disease.
Figure 1. The cervical transformation zone (23).
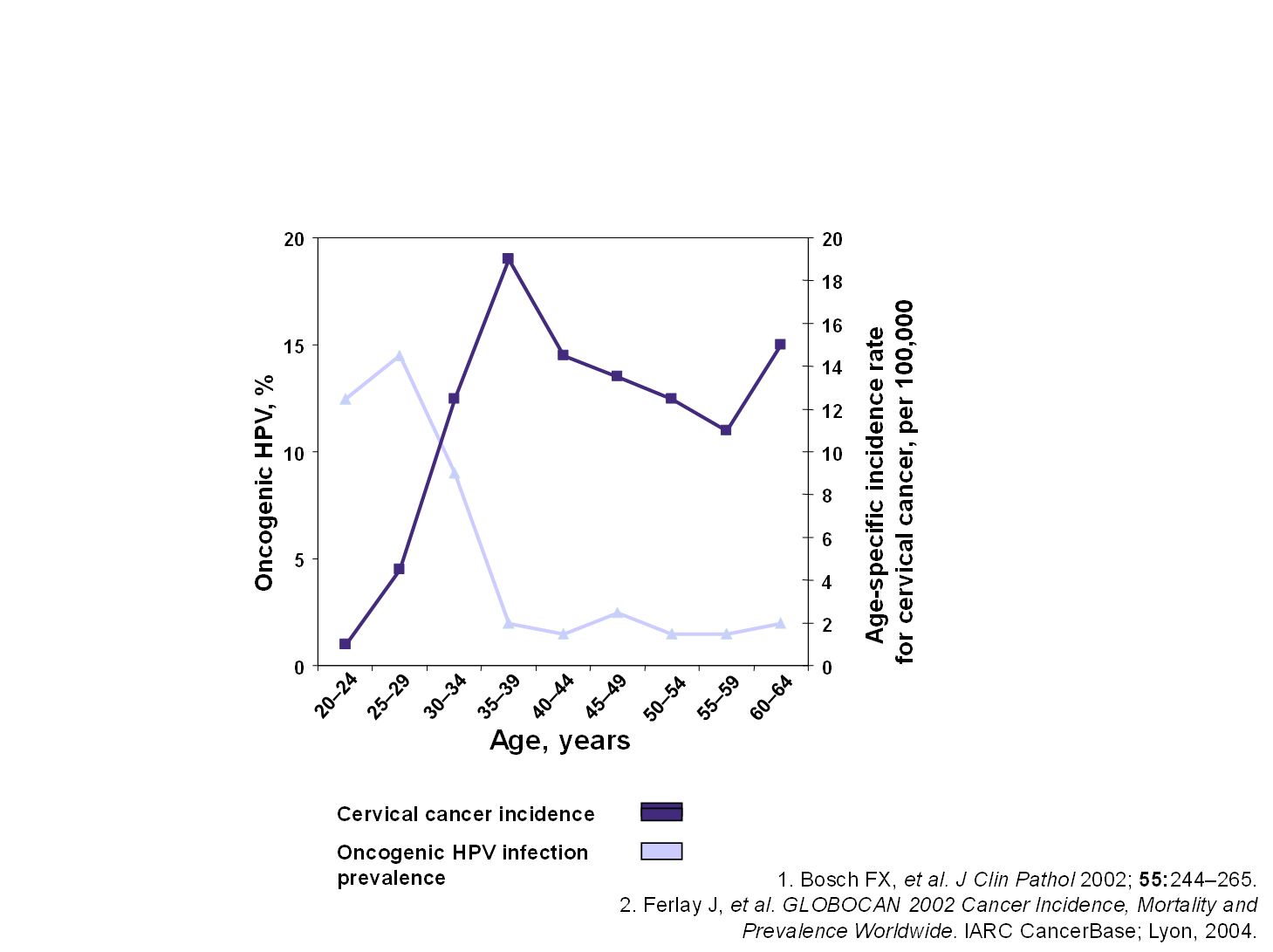
Cervical HSIL may develop within 1-10 years from the time of first infection with “high-risk” HPV types, but the modal time is about 7-10 years (24). Only a small proportion of women with HSIL progress to cancer, and of the women who progress most take a long time to develop invasive disease, which allows for a long interval in which detection can occur and treatment can be given. It is estimated that the risk of invasion is about 20-30% over 5-10 years from HSIL.(25, 26). The prevalence of HPV infection is high in young women, but as the infection is cleared in the majority of women, the prevalence of HPV infection falls while the incidence of cervical cancer rises with increasing age (Figure 2).
Figure 2. Age-specific incidence of cervical cancer and prevalence of oncogenic HPV infection (23)
Most cervical carcinomas are squamous in origin with a smaller proportion being glandular in origin (adenocarcinoma) (27, 28). The prognosis for adenocarcinoma is not as good as for squamous cell carcinoma, with a higher likelihood of recurrence (29). The HPV types most commonly associated with cervical adenocarcinoma are HPV 16, 18 and 45, which account for 90% (30-32). Adenocarcinomas in older women have a lesser association with HPV, being present in only 43% compared to 89% in women under the age of 40 years (27).
Screening
Usually, the precursors of cervical squamous cell carcinoma occur on the ectocervix and are detected by screening for high-risk HPV genotypes followed by colposcopy with visualisation of the lesion, cytology and biopsies (33, 34). In Australia, the Cervical Screening Test (an HPV test) has replaced the Pap test as of 1 December 2017. This test detects high-risk HPV. Screening commences at age 25 and women exit the program by the age of 75. For more details, see (35).
Clinical presentation
Precursor lesions of cervical cancer are usually asymptomatic. Symptoms of cervical cancer can be vaginal bleeding or discharge, weight loss, dyspareunia or unexplained, persistent pelvic and/or back pain.
Diagnosis
Diagnosis requires cytology, colposcopy and biopsy.
Treatment
Current treatment of cervical HSIL is by surgically removing the areas of the cervix that may possibly be involved by laser excision, loop excision or cold coagulation of the cervix. No treatment is currently provided for the HPV infection of the cervix in the absence of dysplasia, even though many of these women will go on to develop cervical dysplasia.
Cervical cancer treatment depends on the stage of the disease and this requires investigation to ascertain whether the disease has spread to the regional pelvic lymph nodes or further. Stage 1 (limited to the cervix) may be treated with surgery with larger tumours requiring radiotherapy and chemotherapy.