HIV shows a high rate of genomic evolution due to the error-prone nature of RT (which introduces random sequence changes into newly produced viral RNA)[23], the high rate of viral production, and the rapid turnover of productively infected cells. For these reasons HIV strains rapidly develop resistance to antiretroviral monotherapy through the acquisition of mutations in RT, envelope or protease genes that confer resistance of enzymatic function to the effects of the drug on the enzyme. The principle behind combination antiretroviral therapy (cART) is to achieve a low level of viral replication and thus a reduced opportunity for the introduction of advantageous mutations into newly produced viruses. Strains that have mutated to become resistant to one therapeutic agent may also have abnormally lowered replicative capacity (fitness), making the acquisition of mutations to further agents less likely.
The resistance profile of a viral strain can be estimated by examination of the nucleic acid sequence of the target genes for evidence of known resistance mutations, or directly assessed by tissue culture of the virus (full length or cloned into a common viral backbone) in the presence of a panel of antiretroviral drugs. Treatment may then be altered in the knowledge that a patient is carrying a virus resistant to one or more agents. Studies have demonstrated improved virological outcomes in patients whose therapeutic choices have been guided by the use of resistance testing[24] [25] [26] [27] [28] [29] [30] and the use of resistance testing is regarded as standard of care in Australia, western Europe and the USA[31] [32].
There are a number of commercially available methods for determining the resistance profile of an HIV isolate. The most common is genotypic resistance testing, which is the only assay routinely available in Australia and is supported by the Medicare Benefits Schedule (MBS). Samples submitted for genotypic antiretroviral resistance testing should be accompanied by a request for a plasma HIV RNA level and a treatment history to aid in the interpretation of test results.
Antiretroviral drug resistance genotyping
Assessment of the HIV genotype (i.e. the nucleic acid sequence) involves the isolation of viral RNA followed by the RT-PCR amplification of portions of the target genes. These amplification products are then sequenced using standardised automated DNA sequencing procedures. Ultracentrifugation of a plasma sample with a low HIV viral load (1000 – 2000 copies/mL) will pellet free virus for RNA extraction and sequencing. Test sequences are compared with a wild-type control reference strain (i.e. no prior exposure to antiretroviral agents) for annotating differences in the predicted amino acid sequences. Mutations that have been associated with resistance to antiretroviral drugs are then identified by comparison with a database of known codon (genetic code) mutations. Resistance mutations are usually reported as primary (generally associated with phenotypically detectable drug resistance) or secondary (mutations generated after the primary mutation, and which may confer varying levels of resistance). The nomenclature of mutations is the wild-type amino acid (using the 20 letter amino acid code)/the amino acid position in the protein/the mutant amino acid e.g. for a change from the wild- type methionine residue at position 46 of protease to isoleucine is denoted M46I. Mutations that involve the insertion of amino acids follow similar nomenclature with the additional amino acids following the residue position. Tables 2 and 3 show HIV resistance mutations to the classes of antiretroviral agents.
Caution must be exercised in the interpretation and use of resistance genotyping data. Two major factors contribute to the complexity of this process: the contribution of minor species and mutational complexity. It is important to realise that genotypic resistance testing gives a snapshot of the dominant viral forms circulating in the plasma at the time of testing. Viral variants with different resistance profiles may circulate at low levels or be present latently in proviral DNA. These may rapidly re-appear and become dominant once the selective pressure of antiretroviral therapy changes. Only minor species that are circulating at substantial levels (above about 20%) may be detected and reported. For this reason, genotypic resistance data must always be interpreted in the light of a thorough history of treatment and previous resistance testing.
Mutations are associated with drug resistance on the basis of in vitro or in vivo data. These data are not always clear and the publication of new evidence means the assignment of mutation to phenotype is being continuously updated. The substantial sequence variability between HIV strains means that it can be difficult to distinguish naturally occurring viral variants from selected mutations that confer an evolutionary advantage, particularly if this advantage is small or secondary to the existence of a primary mutation. When in doubt, consultation with the laboratory performing the assay is strongly indicated.
Table 2. HIV antiretroviral drug resistance mutations: nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) and non-nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) mutations
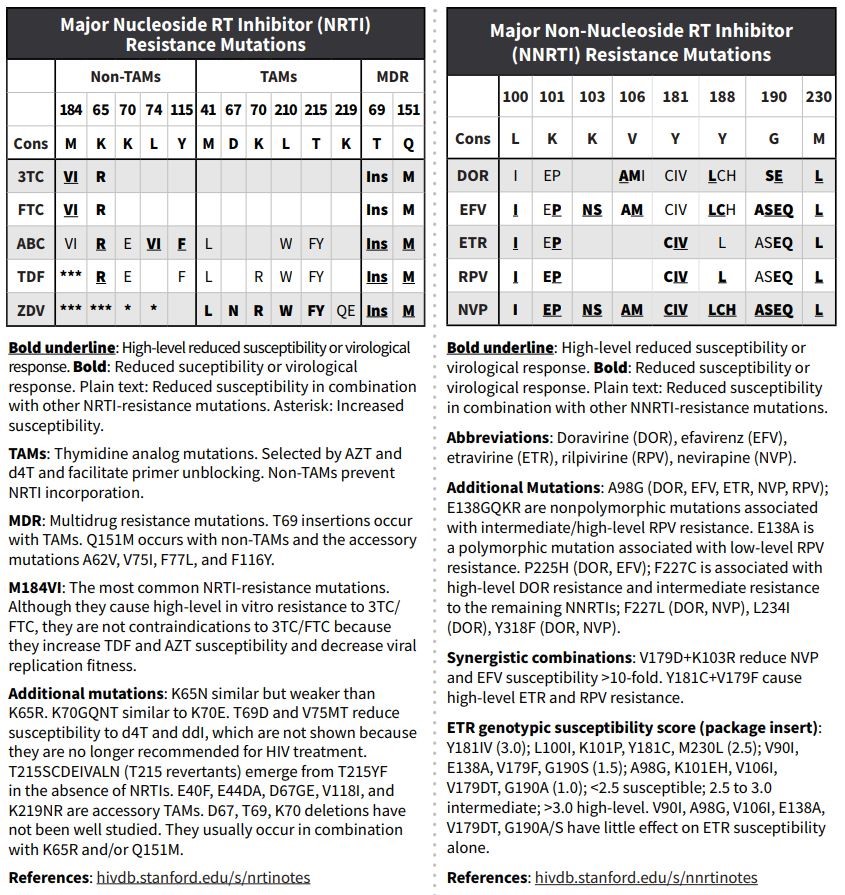
Source: adapted from Standford University HIV Drug Resistance Database. For most current details of interpretation, please refer to http://hivdb.stanford.edu
Table 3. HIV antiretroviral therapy resistance mutations: protease inhibitor and integrase inhibitor mutations.
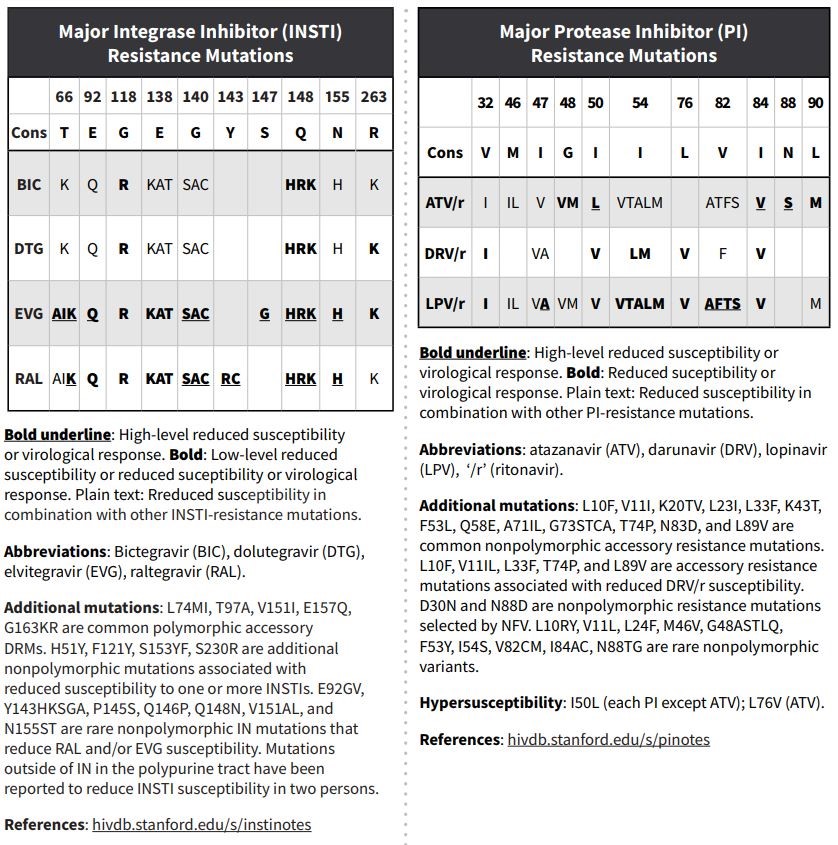
Source: adapted from Standford University HIV Drug Resistance Database. For most current details of interpretation, please refer to http://hivdb.stanford.edu
Resistance phenotyping
Phenotypic drug resistance is considered the gold standard test for drug susceptibility and directly measures the competency of a virus isolate to grow in various concentrations of antiretroviral drugs. Phenotypic drug resistance assays are not routinely performed due to availability, lengthy turn-around time for results and cost. Nucleic acid sequences from the various target genes of HIV are extracted from patient plasma HIV RNA and are inserted into the backbone of a laboratory clone of HIV or used to generate pseudotyped viruses that express the patient-derived HIV genes of interest. Replication competence of the pseudotyped viruses at increasing drug concentrations is monitored by expression of a reporter gene and is compared with replication of a reference wild-type HIV strain. The antiretroviral drug concentration that inhibits viral replication by 50% is calculated, and the ratio of the IC50 (inhibitory concentration) of test and reference viruses is reported as the fold increase in resistance. The addition of phenotypic to genotypic testing is generally preferred for persons with known or suspected complex drug-resistance mutation patterns, particularly to protease inhibitors (PIs)[33].