HIV antibody enzyme immunoassay
Because of its rapidity, sensitivity and low cost, the enzyme immunoassay (EIA) is the standard screening tool for HIV infection[1]. Synthetic and native HIV antigens, fixed on a solid phase, are exposed to and bound by HIV antibodies in test serum. These antibodies are then detected by a second antibody to human IgG, with a sensitivity of more than 99.5%. Most commercially available EIAs are automated and allow for high throughput testing. For example, most laboratories in Australia use testing instrument platforms that enable continuous loading of specimens with results being available within 1 hour. The EIA also detects antibodies against a broad range of HIV types and subtypes, and is continually updated to include newly described HIV-1 subtypes.
Test results arising from the screening (standard) HIV test are classified as reactive or non-reactive (negative) or occasionally invalid. Reactive screening test results must undergo further testing at a designated Reference laboratory to confirm whether the reactivity is true or false. Initially reactive screening results are generally not reported until the confirmatory tests are completed. Test results obtained from the patient sample are compared with a cut-off value which classifies a test as being reactive or negative. In most cases, if a sample is found to be negative by the screening (standard) test no further testing is performed and the result is issued. If acute HIV infection is suspected, other more sensitive tests such as p24 antigen or nucleic acid tests may be indicated. A positive antibody test is usually observed within 3 to 6 weeks following infection. Reactivity on the fourth generation antibody and antigen combination test may be observed several days earlier than antibody-only tests (2-4 weeks).[2]
The weeks between HIV infection and seropositivity are termed the window period and are associated with high levels of circulating HIV RNA, and potentially more efficient HIV transmission. Direct detection of HIV nucleic acids by molecular amplification tests such as polymerase chain reaction (PCR) or serological detection of HIV p24 antigen is usually possible before the detection of HIV antibodies. These direct detection virological tests are indicated in suspected cases of primary infection or seroconversion illness or having a high-risk exposure in the previous 6 weeks and suspected of having acute HIV infection.
False-positive test results are rare and the specificity of most EIAs is above 99.8%. Factors associated with false-positive EIA results are not well characterised and may include antibodies to human leukocyte antigen (HLA) class II antigens, autoantibodies and immune complexes, malaria, recent vaccination and acute viral infections, but also laboratory/technical errors in testing procedure and specimen handling. Therefore, although a negative enzyme-linked immunosorbent assay (ELISA) result, repeated at 3 months, effectively rules out a diagnosis of HIV infection, an initially reactive EIA result is not indicative of infection unless confirmed by supplemental tests including a positive Western Blot assay or nucleic acid test.
HIV rapid tests
The use of HIV rapid tests has gained popularity since their availability in the late 1980s. Rapid HIV tests were first introduced in Australia in 2013 despite being widely available in other countries for many years. These devices are screening tests intended to be performed in settings near or at the side of the patient (hence the name point-of-care HIV tests) and have rapidly become a convenient and highly acceptable form of testing that may lead to increased uptake and frequency of testing when compared with conventional clinic- and laboratory-based testing[3]. Introduction of rapid HIV tests in some countries has been driven by the lack of laboratory infrastructure mainly in resource limited settings but more recently through a growing recognition of the public health benefits of promoting and improving access to individuals who may not otherwise engage in conventional testing pathways. Point-of-care HIV tests generally involve alternate sample types including finger prick capillary blood or oral fluids and provide results in 10 – 30 minutes by visual reading of reactivity to the HIV antigen and the internal control lines. In Australia, it is a requirement that all reactive HIV point-of-care tests be confirmed by conventional diagnostic laboratory tests.
The Australian regulator requires rapid HIV tests to have a clinical sensitivity of 99.5% for whole blood, serum or plasma and 99% for oral fluid tests (based on testing performed outside of the seroconversion window period for the device) and a clinical specificity of at least 99% for detection of HIV infection.[4]
While many rapid tests for HIV infection demonstrate a high level of sensitivity and specificity, it is recognised that most have limitations when compared with conventional tests. The most common limitation is the prolonged window period when detecting the presence of HIV antibodies by simple lateral flow technology. It has also been recognised that operators of rapid HIV tests should undergo comprehensive training in their operation, understand the limitations of the tests and use appropriate key messages and language in the delivery of test results.
Examples of rapid HIV tests are shown in figures 1A-D
Figure 1A. Trinity Unigold HIV-1 antibody test
(NR: valid non-reactive test; R: valid reactive test)
Note two lines C: internal procedural control and T: test line detects presence of HIV antibodies

Figure 1B. Alere Determine HIV-1 and HIV-2 antigen and antibody Ag/Ab combination test
This test presents three lines (control; Ag and Ab)
Test strip marked 10B is a valid reactive test showing control line, antibody (Ab) and weak reactivity to antigen (Ag) lines.
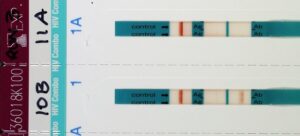
Test strip marked 11A is a valid non-reactive test showing a control line indicating the test is valid, but no reactivity is visible in the Ag or Ab test areas.
Source: NSW State Reference Laboratory for HIV, St Vincent’s Hospital Sydney Limited.
Figure 1C. ATOMO HIV Self Test antibody test

Sample with a HIV negative test result

Sample with a HIV reactive test result
Source: Atomo Diagnostics
The Atomo HIV Self Test is a single-use, immunochromatographic, rapid in-vitro diagnostic test for the detection of antibodies to Human Immunodeficiency Virus Type 1 (HIV-1) and Type 2 (HIV-2) in whole blood.
The Atomo HIV Self Test is intended to be used by untrained lay users in a private setting as a self test to aid in the diagnosis of infection with HIV-1 and HIV-2 from samples of fresh, whole blood obtained through a finger stick blood collection technique. The device requires a sample size of 10uL.
The Atomo HIV Self Test is comprised of a test strip inside a plastic cartridge. The test is performed by placing a small drop of blood on the test strip and then applying drops of test fluid (diluent). When the test is completed, two lines can appear on the strip. The control line will only become visible if the test has been performed correctly. The test line will only become visible if the applied sample contains antibodies to HIV.
Figure 1D. Orasure OraQuick Advance HIV 1 / 2 test

The Orasure device is the only product on the Australian market that detects HIV-1 and HIV-2 antibodies in oral fluids as well as plasma/serum or whole blood from venepuncture or fingerstick. While the test is available as over the counter self-testing applications in other countries (such as USA) it is not available in Australia for home or self-testing.
HIV-1 Western Blot assay
The Western Blot assay involves detection of antibodies in patient sera that react with a number of different HIV proteins. These proteins are separated into bands of distinct molecular weight using protein gel electrophoresis. After transfer (blotting) to a solid membrane, proteins that bind HIV antibodies in test sera can be identified. Antibodies to different HIV-1 proteins appear in a defined order. First, antibodies to the structural gag proteins, the precursor (p55), p24 and p18, appear. These antibodies are closely followed by antibodies to the envelope glycoproteins – the precursor gp160, the extracellular gp120, the transmembrane gp41 – and then the polymerase components p31, p51 and p66. Antibodies to the smaller regulatory and accessory HIV proteins encoded by Vpr, Vpu, Vif, Rev, Tat and Nef may also be seen.
The Western Blot test is classified as negative if there is no reaction of the patient’s serum with any HIV protein bands. An individual is classified as seropositive for HIV antibodies according to specific criteria. There is a lack of consistent interpretation criteria defined by the different peak organisations Centers for Disease Control and Prevention [CDC], World Health Organization [WHO], Consortium for Retrovirus Serology Standardization (CCRS), which has led to confusion about classification of HIV seropositive samples. Generally, a positive Western Blot result is defined by the detection of antibodies to all of the three main groups of HIV proteins – envelope (gp160, gp120 or gp41), gag (p24, p55) and polymerase (p68 or p51). The WHO criterion for a positive Western Blot is a minimum of two envelope glycoproteins. Samples that do not meet the criteria for seropositivity but demonstrate reactivity to some viral proteins are classified as indeterminate. Previously, HIV Reference Laboratories in Australia interpreted Western Blots according to National Serology Reference Laboratory criteria, where there were four groups of indeterminate Western Blots profiles each corresponding to the likelihood of HIV infection with reactivity profiles containing antibodies to envelope glycoproteins being the most specific or most likely to be associated with true HIV infection.
In some countries, including the USA, the HIV-1 Western Blot test is being replaced by HIV-1/2 confirmatory assays such as the Bio-Rad Geenius™ HIV 1/2 Confirmatory Assay. Any indeterminate result is then referred for nucleic acid-based testing. In Australia however, reference laboratories are experienced in interpretation of Western Blot results and many experts believe it is important to retain a native HIV viral protein assay in the testing strategy to safeguard against possible false-negative results arising from HIV genetic diversity if nucleic acid-based tests are used. However, there is great interest in the pathology sector regarding emerging nucleic acid tests for HIV diagnosis.
Figure 2. Typical appearance of an evolving HIV-1 Western Blot in HIV infection (seroconversion)

Note: serial Western Blot test strips exposed to serum from the patient demonstrating the typical stepwise appearance of bands to the specific viral antigens over time.
Source: NSW State Reference Laboratory for HIV, St Vincent’s Hospital Sydney Limited.
An indeterminate Western Blot assay should be followed by repeat HIV serology tests after 4 to 6 weeks, to exclude an evolving HIV antibody response. During seroconversion (changing from seronegative to seropositive) the evolving pattern of antibody/viral protein bands is dynamic with additional bands occurring in days to weeks following infection. The application of tests that directly detect the presence of viral nucleic acid or protein (p24) may be used, especially when the index of suspicion is high. A positive result in one or more such assays leads to a presumptive diagnosis of HIV infection, pending the development of a Western Blot assay which meets positive criteria for HIV antibodies. Negative results from one or more of these assays, and a non-evolving indeterminate Western Blot assay, exclude HIV infection and indicate that the initial reactivity on the screening test is non-specific or false. These results are frequently called biological false positives (BFP).